You stare at one trashed HDL or one ugly LDL number on cycle and act like that single line tells the whole story. It doesn’t. On cycle, HDL usually drops, LDL often climbs, and if you’re shocked by that, you’re already late.
What I care about is how bad the whole picture is, how long you stay there, and what you do next. I don’t waste time with panic over one screenshot when the bigger risk stack is sitting right in front of you.
The Problem
If you’re using anabolics, your lipids usually get uglier. That’s normal in the sense that it happens a lot, not normal in the sense that it’s harmless. Steroids can mess with how the liver handles blood fats, so HDL falls and LDL rises, sometimes fast, sometimes within days to weeks. Oral compounds usually hit harder than many injectables, and that part matters.
A low HDL is common on cycle, but I don’t ignore it. HDL helps move cholesterol out of circulation and back toward the liver. When it gets crushed, you lose some of that cleanup crew. Research on the atherogenic effects of anabolic steroids on serum lipids has shown some pretty nasty swings, especially in users pushing harder compounds.
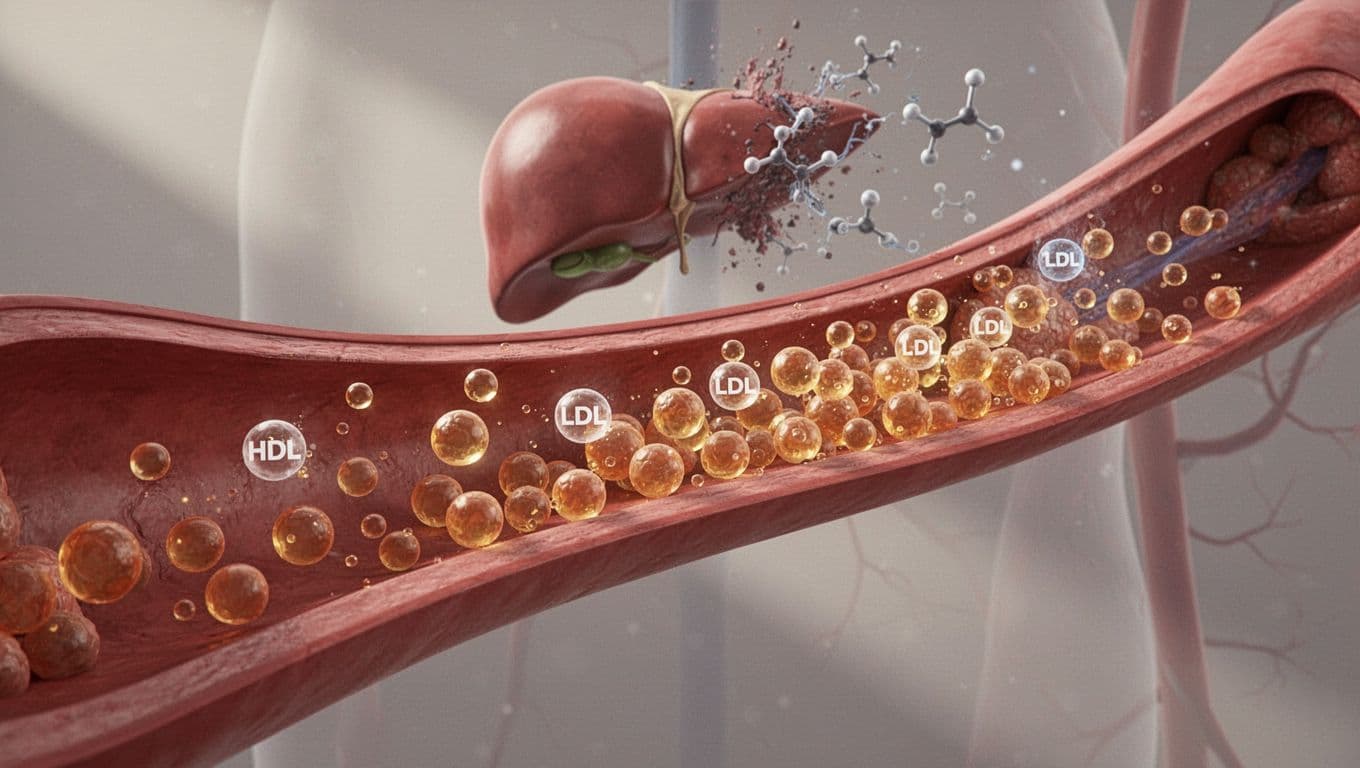
LDL matters too, because LDL particles are part of what gets driven into artery walls over time. One rough week is one thing. Staying high for months, while blood pressure, body fat, and hematocrit are also climbing, that’s where dumb shit turns expensive.
The Reframe
This is where most guys screw it up. They reduce heart risk to HDL versus LDL like it’s a boxing match and whoever wins the ratio gets a free pass. No. I care more about pattern, exposure, and stacked risk than one basic panel.
If I can get ApoB, I care about that more than HDL alone, because ApoB is closer to a count of the problem particles. Think of it like traffic. I don’t only care how much junk is inside each car, I care how many cars are on the road heading toward the same wall. Non-HDL cholesterol helps too when ApoB isn’t there.
One bad marker is a warning. A pile of bad markers is a plan to get hurt.
I also want triglycerides, blood pressure, hematocrit, fasting glucose or A1c when it fits, cardio fitness, body fat, family history, and time on cycle. Lp(a) matters because it can show inherited risk your basic panel misses. The research on apolipoproteins and lipoprotein(a) is useful here, because some people look average on standard labs and still carry extra risk in the background.
What I Actually Look At
When I review cycle bloodwork, I don’t play the screenshot game. I want trend lines. Pre-cycle, mid-cycle, post-cycle. That’s how I see whether you’re taking a temporary hit or driving the car into a ditch with your eyes open.
First, I look at LDL, HDL, non-HDL, and triglycerides. If ApoB is there, great, I lean on it hard. If it’s not, I still get a solid picture from the rest. I also look at blood pressure, because bad lipids with high pressure is a worse story than bad lipids alone. Then hematocrit, because thicker blood doesn’t magically become fine because your bench went up.
After that, I check glucose control, liver enzymes, and kidney markers. Not because this is a nerd hobby, but because risk stacks. A guy with beat-up lipids, rising ALT and AST, poor fasting glucose, shit cardio, and a sloppy bulk is not “fine because he’s young.” He’s collecting problems.
I also care about bodyweight trend and waist gain. If you’re up fast, puffy, out of breath, and eating like a raccoon behind a gas station, don’t pretend the lab sheet is the only issue. More fat gain, worse insulin sensitivity, worse blood pressure, worse sleep, maybe sleep apnea too. Now the lipid problem sits in bad company.
Then I ask the simple stuff. What compounds? What dose? How long? Orals often hammer lipids harder, and the old data comparing testosterone and stanozolol on lipoproteins makes that point pretty damn clearly. Exposure matters. A moderate hit for a short window is not the same as months of abuse with stacked compounds and no brakes.
I don’t freak out over one weird test from one bad week either. Hydration, illness, trash food, timing, even a stupid weekend can muddy the picture. But repeated bad trends are different. If HDL stays crushed, LDL or non-HDL stays high, triglycerides climb, and blood pressure is drifting up, I’m not waiting around for magic.
Yes, some of this improves after the cycle ends. That does not make reckless exposure smart. “It’ll bounce back” is the same logic guys use right before they need a bigger problem to finally listen. If you want the coaching side of how I structure this stuff, read the protocol.
What To Do Instead
Stop acting like fish oil is a force field. Omega 3s can help, sure, but they don’t erase a reckless cycle, zero cardio, fast food, low fiber, bad sleep, smoking, and 25 pounds of sloppy gain.
Clean up the obvious garbage first. Eat like an adult. Get more fiber in. Walk more. Do your cardio even when you don’t feel like it. Keep body fat under control. Pick smarter compounds. Use lower doses when possible. Keep exposure shorter. Get repeat labs before, during, and after. If the numbers are getting hammered, adjust early or stop bullshitting yourself. If you want more straight talk on this stuff, read more articles.
If your HDL is buried, your LDL is climbing, and the rest of the picture looks worse by the month, don’t hide behind “I’m only on a little bit.” That’s kid logic. Be a grown man, look at the full risk picture, and act like it. If you want help sorting the signal from the noise, work with me.
Feel good, eat good, fuck good.
Disclaimer This article is for education only. It is not medical advice, diagnosis, or treatment. If you have a medical condition, take medication, use PEDs, or have abnormal labs, get qualified medical oversight before applying any of this.
Author Angelo is a European online coach and a former competitive bodybuilder. He works with serious lifters who want more muscle, better condition, sharper execution, and less guesswork. The job is simple: fix the basics, apply progression properly, manage recovery, and stop doing dumb shit that kills progress.
Scientific References