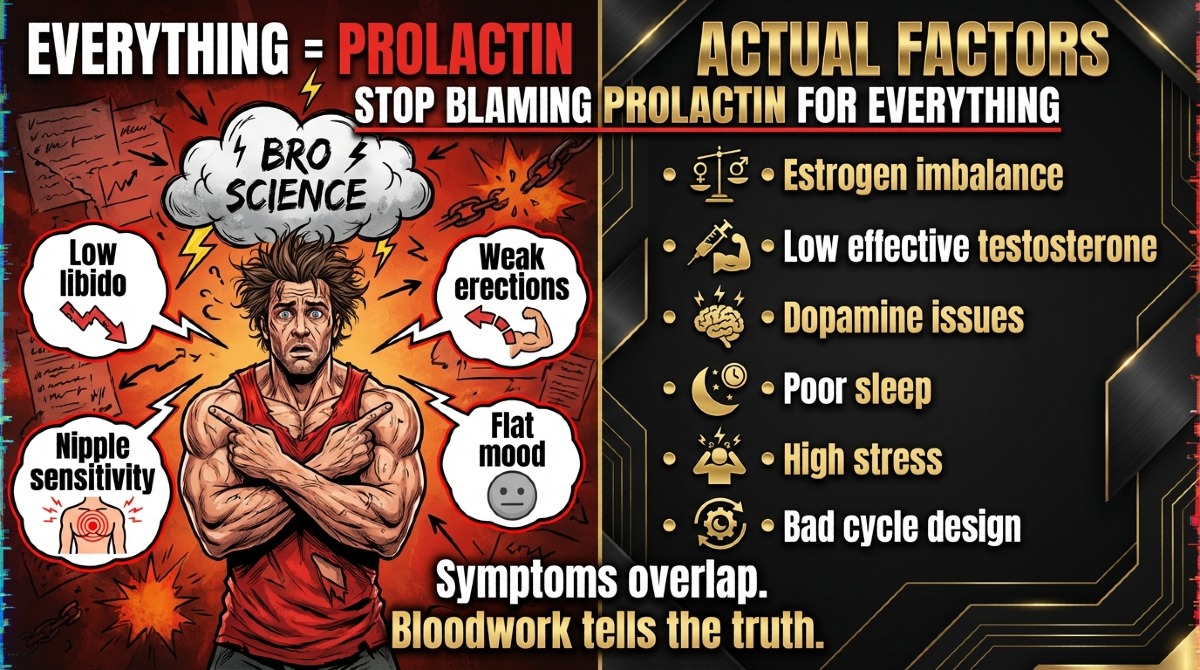
Stop blaming prolactin for every damn thing the second Deca or Tren shows up.
I see this all the time. Libido drops a bit, erections get weird, nipples feel spicy, mood goes flat, and guys instantly scream “high prolactin” like they solved the case. Most of the time, they didn’t solve shit. Estrogen is off, testosterone is buried, dopamine is in the gutter, sleep sucks, stress is high, and the cycle was built like trash. That’s the real conversation.
The Problem
The prolactin story got huge because bodybuilding loves a simple villain. “Deca dick” became a campfire story, then Tren got thrown in the same bucket, and now half the internet treats a meme like lab work. You can see it in a typical forum thread like this, where symptoms get labeled before anyone even asks for bloods.
That’s the trap. Guys confuse symptom overlap with proof. Low libido, weak erections, trouble finishing, flat mood, nipple sensitivity, all of that can happen from high estrogen, low effective testosterone, stress, bad sleep, anxiety, or a cycle setup that makes no sense. Similar symptoms do not mean the same hormone problem. Also, people hear that 19-nors have progestin-like activity, then they oversimplify it into “therefore prolactin is the issue.” That leap is where the bullshit starts.
The Reframe
Here’s the better way to think about it. Deca and Tren do not automatically mean your prolactin is high. That’s too clean, too easy, and usually too dumb. The real-world picture is messier. Some users do show elevated prolactin, especially in ugly stacks or after long abuse, but it’s not a law of nature tied to the drug name alone.
I like this breakdown of prolactin and steroid use for one reason, it at least treats the topic like a hormone problem that needs context, not a ghost story. True prolactin problems are more often tied to bigger medical issues, certain meds, thyroid trouble, or a full endocrine mess, not “I injected Tren, therefore prolactin attacked me.”
If your symptoms fit ten possible causes, you don’t get to call one of them the winner without labs.
What I Actually Look At
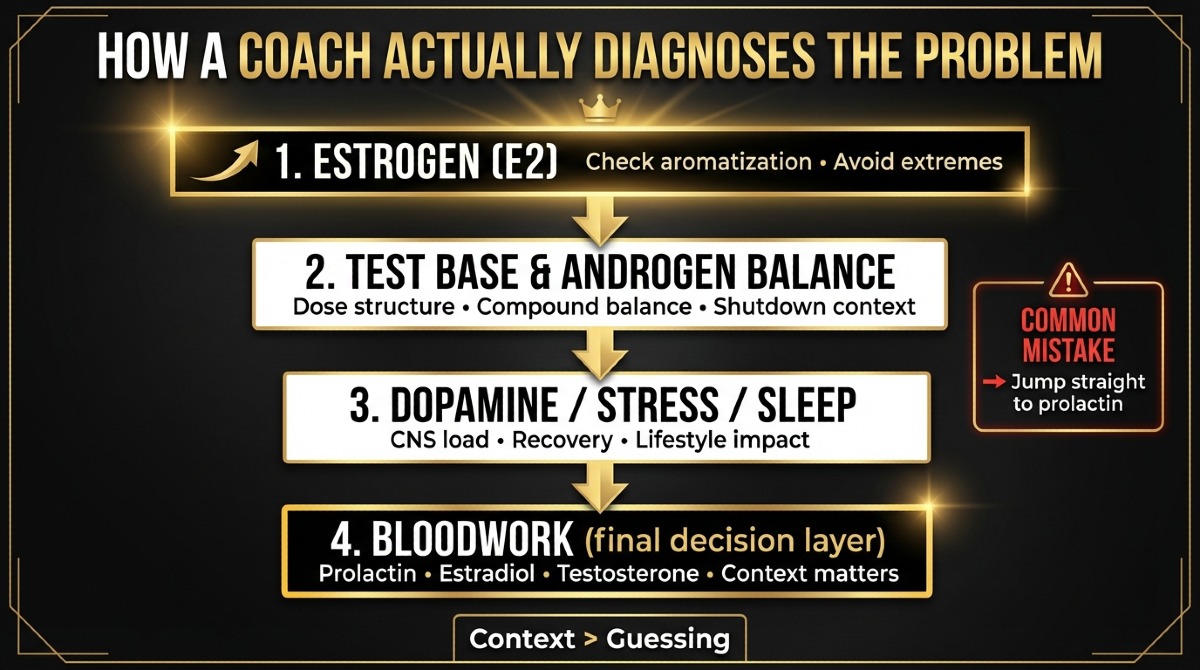
This is where coaching beats bro lore. I don’t start with the scary story. I start with the setup.
Estrogen comes first. A lot of guys are running enough testosterone to aromatize hard, then they either ignore estrogen or crush it like idiots. High E2 can bring water retention, mood swings, gyno panic, softer erections, and a weird up-and-down sex drive. Then they blame prolactin because that sounds edgy. No. A messy estrogen picture causes a ton of the same chaos, and I see it way more often.
Then I look at the test base and the whole androgen balance. If your natural production is shut down and your cycle has a weak test base, poor dose balance, or random compounds stacked on top, sexual function can get cooked fast. Deca or Tren on top of weak overall planning can make you feel like hell. That doesn’t prove prolactin is the star of the show. It often proves the cycle was built by a guy who learned endocrinology from gym bathrooms.
Then I look at dopamine, stress, sleep, and nervous system strain. This part gets ignored because it’s not sexy. Tren especially can hammer sleep, increase anxiety, and leave you wired but dead inside. That changes arousal, orgasm, drive, patience, and mood. Add high stimulants, hard training, low food, relationship stress, and zero recovery, and now you’ve got a whole pile of problems that look hormonal even when prolactin isn’t the main driver. Sometimes prolactin rises in that mess, sure, but it’s part of the mess, not always the cause.
Last, bloodwork decides the conversation. I want prolactin, estradiol, total testosterone, free testosterone if it makes sense, and sometimes thyroid markers if the symptom picture is ugly enough. I care about timing, doses, how long you’ve been on, sleep quality, appetite, stress, stimulants, and whether you’re reading the labs like a sane person. If you want a general checklist, for example this mid-cycle lab guide is a decent starting point. The point is simple, I don’t medicate a myth. I match labs plus symptoms plus context.
What To Do Instead
Don’t self-diagnose off nipple paranoia and a bad week in bed. Clean up the cycle. Look at estrogen management. Look at the test-to-19-nor balance. Fix your sleep. Calm the stimulant abuse. Stop training like a lunatic when recovery is already wrecked.
Then pull bloods before you touch caber. Cabergoline has real downsides, and I hate how casually guys throw it in. It’s not candy. It’s not a magic eraser. If you like the way I troubleshoot this stuff, read the protocol and see how I think through the whole system.
Deca and Tren can bring real side effects, no question. I just don’t use prolactin as a lazy answer for every problem under the sun. If you want me to look at the whole picture instead of guessing, work with me.
Feel good, eat good, fuck good.
Disclaimer This article is for education only. It is not medical advice, diagnosis, or treatment. If you have a medical condition, take medication, use PEDs, or have abnormal labs, get qualified medical oversight before applying any of this.
Author Angelo is a European online coach and a former competitive bodybuilder. He works with serious lifters who want more muscle, better condition, sharper execution, and less guesswork. The job is simple: fix the basics, apply progression properly, manage recovery, and stop doing dumb shit that kills progress.